OH NO OZEMPIC: How GLP-1 RAs May Be Slimming Down Your Oral Health
- Aug 3, 2025
- 8 min read
Updated: Sep 10, 2025
Sooyun Christina Kim, Amreet Minhas, Beatrice Sixt
Project Smile Global
August 3, 2025

In recent years, Ozempic, a medication used to treat type 2 diabetes mellitus (T2DM), has increased in popularity (Callaghan et al. 2). Besides T2DM, the use of this drug has skyrocketed due to its ability to aid weight loss (Callaghan et al. 2). Given the prevalence of obesity worldwide, along with societal expectations regarding health and physical appearance, it is evident that Ozempic is a sought-after medication (Han et al. 60). While research demonstrates how Ozempic can be beneficial for treating both T2DM and obesity, widespread use of this drug has been associated with several health concerns (Mansour et al. 225). These include nausea, gastrointestinal issues, and changes in skin volume (Mansour et al. 225). Additionally, it has been reported that certain oral health risks are associated with using Ozempic, including halitosis, dry mouth, and changes in taste (Bando 18). On the contrary, some studies suggest that use of this drug can also reduce inflammation associated with periodontitis (an inflammatory disease of the gums), among other benefits to oral health (Yaribeygi et al. 1; Sawada et al. 2; Basha et al. 3375). Despite the multitude of risks and benefits that have been reported, the effects of Ozempic use are still being explored, given the implications of weight loss in a relatively short time period, and how several systems in the body can be affected (Suran 1628).
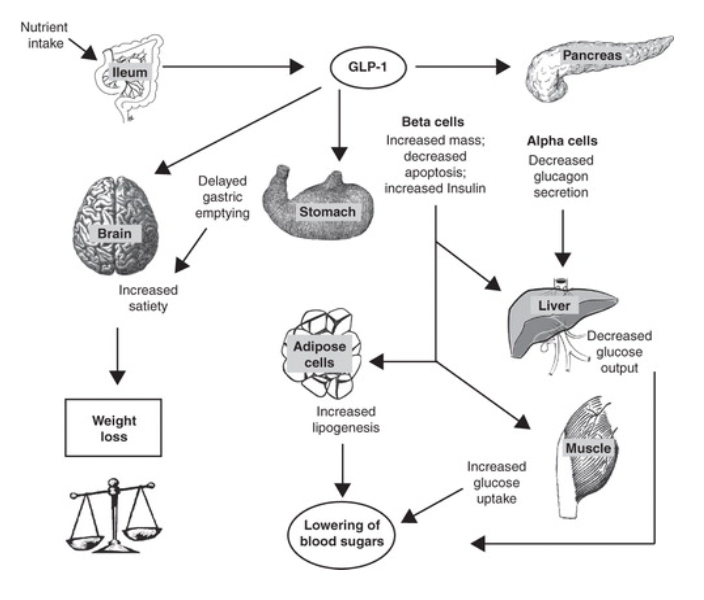
Ozempic is part of a larger class of drugs known as glucagon-like peptide-1 receptor agonists (GLP-1 RA), which are gut-derived incretin hormones (Muskiet et al. 605). GLP-1 can stimulate insulin production in pancreatic beta-cells, suppress glucagon in pancreatic alpha-cells, reduce appetite signalling from the brain, and slow down gastric emptying in the stomach, all of which work in conjunction to decrease blood glucose levels (Nauck 852). Subsequently, it is used as treatment for T2DM patients, as they experience insulin deficiency due to high blood glucose levels (Garber 46). However, due to GLP-1’s short-term metabolic effects, “agonists” are utilized as they mimic the effects of GLP-1 long-term, such as binding the receptors that GLP-1 normally binds to, and have shown promising results in treating type 1 diabetes mellitus as well (Mohandas et al. 94).
Apart from GLP-1 RA’s positive effects on lowering blood pressure and glucose, and promoting weight loss, it has several other benefits. Liraglutide, a GLP-1 analogue (a compound with similar effects as GLP-1), was found to lower morbidity rates from cardiovascular causes (Marso et al. 311). Similar studies have suggested that GLP-1 RAs also have protective effects on the kidney, which can potentially be used to treat diabetic kidney disease (DKD) (Yu et al. 136). Interestingly, liraglutide was found to ameliorate the development of periodontitis, an inflammatory disease of the gums, by reducing M1 macrophages, which are involved in the inflammatory response (Sawada et al. 7). Diabetes and periodontitis have a complex bidirectional relationship, as risk for periodontitis is two to three times higher in diabetes patients (Preshaw and Bissett. 577). Further in-vitro studies have found other GLP-1 RAs, such as exenatide, to promote osteogenic differentiation of periodontal ligament stem cells, which mitigate periodontal inflammation, promoting bone remodeling and combatting periodontitis (Ahmad et al. 1). While these emerging studies provide promising results, they note that GLP-1 RAs are more effective in, “preserving periodontal and peri-implant health in T2DM patients than in directly treating periodontitis or peri-implantitis” (Ahmad et al. 12).

Conflictingly, there is growing evidence to suggest that Ozempic and other GLP-1 RAs have detrimental effects on oral health. Many patients report dry mouth (xerostomia), enamel erosion, inflamed gums, and even cracked or loose teeth after taking Ozempic (Schimelpfening). Although this phenomenon has not been recognized as a clinical diagnosis, many refer to it as “Ozempic teeth,” following similar attempts to label GLP-1 RA side effects such as “Ozempic face” and “Ozempic butt” (Schimelpfening). Recent studies have reported cases of semaglutide-associated hyposalivation (a type of GLP-1 RA), where patients experienced minimal salivation and xerostomia, which dissipated as soon as they discontinued taking the GLP-1 RA (Mawardi et al. 2). Other studies have supported this finding, as GLP-1 RAs induced apoptosis (cell death) and oxidative injury in mice salivary glands (Kim et al. 139). Additionally, one study reported increased dysgeusia (loss of taste), throat tightness and irritation, dysphagia (difficulty swallowing), and dysphonia (difficulty speaking) (Khan et al. 3). Similarly, as previously outlined, some studies have suggested positive effects of GLP-1 RAs on bone cells, turnover, and bone density, but human studies have yielded either no significant or limited results regarding their impact on bone mineral density and fracture risk (Viggers et al. 1). While liraglutide has been a popular choice of drug, no data has been reported in preclinical trials with semaglutide, and most of the positive effects on bone density and microarchitecture were observed at concentrations much higher than approved for obesity treatment in humans (Herrou et al. 86). Overall, the effects of GLP-1 RAs on fracture risk, salivation, and the other oral health parameters may vary depending on the choice of drug and the follow‐up duration (Viggers et al. 1).
The surge in popularity of Ozempic sheds light on the impact of socioeconomic factors in accessing the drug. Ozempic and other GLP-1 RAs are significantly more difficult to access for those from lower-income communities, due to factors such as base price and insurance coverage. Ozempic alone costs $935 per dose per month without insurance (Shah 35). For reference, one dose is meant to be administered per week. The high price tag makes insurance essential in accessing the drug. However, a higher percentage of individuals from low socioeconomic status communities lack medical insurance and receive poorer quality healthcare. Black, Indigenous, and People of Color (BIPOC) and low-income families are more likely to be uninsured or receive Medicaid benefits, the latter of which many healthcare providers do not accept. A study found that many participants reported traditional barriers to medical care, such as high cost (24.1%) and no health insurance (8.3%) (Taber et al.). Such factors further prevent or discourage low SES patients from accessing the limited supply of GLP-1 RAs. However, low SES communities are among those most in need of GLP-1 RAs. In a study concerning the link between diabetes risk in US adults and SES, participants with lower SES were found to have a higher risk of diabetes compared to those with a higher SES (Liu, Ce et al.).
GLP-1 RA medications, such as the popular Ozempic, intend to treat T2DM and obesity by simultaneously stimulating insulin production and suppressing appetite and glucagon to decrease blood sugar levels. As aforementioned, however, there are mixed reports on the drugs’ impact on patients’ oral health. Many patients have reported dry mouth, enamel erosion, inflamed gums, and even cracked or loose teeth. Those with low socioeconomic status, who experience diabetes risk at a higher rate, face significant barriers to accessing GLP-1 RAs due to the high cost of the drug combined with lower rates of insurance.
Overall, while Ozempic and related drugs boast multiple benefits for those affected by T2DM and obesity, these medications present a complicated set of side effects which are still being researched. In terms of oral health effects, studies highlight both potential benefits, such as reduced gum inflammation, and detrimental effects, including weakening of enamel and decreased salivary function. Additionally, access to these medications remains a cause for concern, especially for low-income and marginalized communities. These populations are disproportionately affected by diabetes, yet face barriers to care as a result of high costs and shortages of Ozempic due to its popularity as a weight-loss drug. This can limit access to those who may rely on the drug to manage T2DM.
Works Cited
Ahmad, Paras, et al. “Glucagon‐Like Peptide 1 Receptor Agonists (GLP ‐ 1RAs) Improve Periodontal and Peri‐Implant Health in Type 2 Diabetes Mellitus.” Journal of Periodontal Research, vol 60, no. 5, 9 May 2025, pp 450-65, https://doi.org/10.1111/jre.13410.
Bando, Hiroshi. “Possible Adverse Effects (AES) of Semaglutide (Ozempic) Administration for the Latest Investigation.” Diabetes Research: Open Access, vol. 5, no. 1, 2 Nov. 2024, pp. 17–20, https://doi.org/10.36502/2024/droa.6189.
Basha, Soha M., et al. “Assessment of Semaglutide Therapy on Inflammatory Mediators in Diabetic Rats with Experimental Periodontitis.” Egyptian Dental Journal, vol. 70, no. 4, 1 Oct. 2024, pp. 3367–77, https://doi.org/10.21608/edj.2024.309230.3143.
Callaghan, Timothy, et al. “The Prevalence and Consequences of Support for Off-label Ozempic Prescriptions.” Health Economics, Policy, and Law, 7 Jan. 2025, pp. 1–14, https://doi.org/10.1017/s1744133124000306.
Garber, Alan J. “Novel GLP-1 Receptor Agonists for Diabetes.” Expert Opinion on Investigational Drugs, vol. 21, no. 1, Jan. 2012, pp. 45–57, https://doi.org/10.1517/13543784.2012.638282.
Garber, Alan J. “The effects of GLP-1 on multiple organ systems.” Expert Opinion on Investigational Drugs, vol. 21, no. 1, Jan. 2012, pp. 45–57, https://doi.org/10.1517/13543784.2012.638282.
Han, Sabrina H, et al. “Public Interest in the Off-label Use of Glucagon-like Peptide 1 Agonists (Ozempic) for Cosmetic Weight Loss: A Google Trends Analysis.” Aesthetic Surgery Journal, vol. 44, no. 1, 4 July 2023, pp. 60–7, https://doi.org/10.1093/asj/sjad211.
Herrou, Julia, et al. “Narrative Review of Effects of Glucagon-Like Peptide-1 Receptor Agonists on Bone Health in People Living with Obesity.” Calcified Tissue International, vol. 114, no. 2, 24 Nov. 2023, pp. 86–97. Springer Link, https://doi.org/10.1007/s00223 023-01150-8.
Khan, Faizaan I., et al. “Otolaryngologic Side Effects of GLP ‐1 Receptor Agonists.” The Laryngoscope, 12 Feb. 2025, pp. 1-8. DOI.org (Crossref), https://doi.org/10.1002/lary.32061.
Kim, Hyung Rae, et al. “Effect of Glucagon-like Peptide 1 on Salivary Gland Hypofunction in Diabetic Db/Db Mice.” Journal of Biomedical and Translational Research, vol. 24, no. 4, 2023, pp. 139–50, https://doi.org/10.12729/jbtr.2023.24.4.139.
Liu, Ce, et al. “Diabetes risk among US adults with different socioeconomic status and behavioral lifestyles: evidence from the National Health and Nutrition Examination Survey.” Frontiers in Public Health, vol. 11, 22 Aug. 2023, pp. 1-12, https://doi.org/10.3389/fpubh.2023.1197947
Mansour, Meghan R., et al. “The Rise of ‘Ozempic Face’: Analyzing Trends and Treatment Challenges Associated With Rapid Facial Weight Loss Induced by GLP-1 Agonists.” Journal of Plastic, Reconstructive & Aesthetic Surgery, vol. 96, Sept. 2024, pp. 225–7, https://doi.org/10.1016/j.bjps.2024.07.051.
Marso, Steven P., et al. “Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes.” New England Journal of Medicine, vol. 375, no. 4, July 2016, pp. 311–22, https://doi.org/10.1056/NEJMoa1603827.
Mawardi, Hani Haytham, et al. “Semaglutide-Associated Hyposalivation: A Report of Case Series.” Medicine, vol. 102, no. 52, Dec. 2023, pp. 1-4, https://doi.org/10.1097/MD.0000000000036730.
Mohandas, Deene, et al. “Evaluating the Efficacy and Safety of Long-Acting GLP-1 Receptor Agonists in T1DM Patients.” Endocrines, vol. 4, no. 1, Feb. 2023, pp. 93–101, https://doi.org/10.3390/endocrines4010008.
Muskiet, Marcel H. A., et al. “GLP-1 and the Kidney: From Physiology to Pharmacology and Outcomes in Diabetes.” Nature Reviews Nephrology, vol. 13, no. 10, Oct. 2017, pp. 605–28,https://doi.org/10.1038/nrneph.2017.123.
Nauck, M. A. “Glucagon-like Peptide 1 (GLP-1) in the Treatment of Diabetes.” Hormone and Metabolic Research, vol. 36, no. 11/12, Nov. 2004, pp. 852–58,https://doi.org/10.1055/s 2004-826175.
Schimelpfening, Nancy. “‘Ozempic Teeth’: GLP-1 Drugs May Cause Tooth Decay, Experts Say.” Healthline, 5 June 2025, https://www.healthline.com/health-news/ozempic-teeth may-impact-dental-health.
Suran, Melissa. “As Ozempic’s Popularity Soars, Here’s What to Know About Semaglutide and Weight Loss.” JAMA : The Journal of the American Medical Association, vol. 329, no. 19, 2023, pp. 1627–29, https://doi.org/10.1001/jama.2023.2438.
Preshaw, Philip M., and Susan M. Bissett. “Periodontitis and Diabetes.” British Dental Journal, vol. 227, no. 7, Oct. 2019, pp. 577–84,https://doi.org/10.1038/s41415-019-0794 5.
Preshaw, Philip M., and Susan M. Bissett. “Potential mechanisms linking periodontitis and diabetes, and the impact of periodontal therapy on diabetes control.” British Dental Journal, vol. 227, no. 7, Oct. 2019, pp. 577–84,https://doi.org/10.1038/s41415-019-0794 5.
Shah, Sakhi. Washington , D.C., 2024, pp. 32–35, Addressing the Medicare Weight-Loss Drug Coverage Debate.
Sawada, Noritaka, et al. “Glucagon-Like Peptide-1 Receptor Agonist Liraglutide Ameliorates the Development of Periodontitis.” Journal of Diabetes Research, edited by Yoshifumi Saisho, vol. 2020, Nov. 2020, pp. 1–9, https://doi.org/10.1155/2020/8843310.
Taber, Jennifer M., et al. “Why Do People Avoid Medical Care? A Qualitative Study Using National Data.” Journal of General Internal Medicine, vol. 30, no. 3, 12 Nov. 2014, pp. 290–7, https://doi.org/10.1007/s11606-014-3089-1
Viggers, Rikke, et al. “Effects of Incretin Therapy on Skeletal Health in Type 2 Diabetes—A Systematic Review.” JBMR Plus, vol. 7, no. 11, Nov. 2023, pp. 1-26,, https://doi.org/10.1002/jbm4.10817.
Yaribeygi, Habib, et al. “Anti-Inflammatory Benefits of Semaglutide: State of the Art.” Journal of Clinical & Translational Endocrinology, vol. 36, June 2024, pp. 1–6, https://doi.org/10.1016/j.jcte.2024.100340.
Yu, Ji Hee, et al. “GLP-1 Receptor Agonist in Diabetic Kidney Disease: Current Evidence and Future Directions.” Kidney Research and Clinical Practice, vol. 41, no. 2, Mar. 2022, pp. 136–49. PubMed Central, https://doi.org/10.23876/j.krcp.22.001.

